A major incident is an incident (or series of incidents) causing casualties on a scale beyond the normal resources of the emergency and healthcare services’ ability to manage. The Major Incident Medical Management and Support (MIMMS) manual states that a major incident has occurred “when the location, number, severity or type of casualty requires extraordinary resources.”
A major incident may involve hundreds or thousands of casualties with a range of injuries, the response to which will be beyond the capacity of normal major incident procedures to cope and require further measures to appropriately deal with the casualty numbers. This sort of incident is sometimes referred to as ‘the big bang incident’, examples being a train crash, industrial explosion or terrorist attack.
A major incident can also be declared due to a combination of several smaller incidents or can occur over a long period and build slowly, for example, an infectious disease pandemic. There is also variability between hospitals, a smaller hospital with limited resources being much more easily overwhelmed than a larger hospital with more significant resources at its disposal.
Emergency preparedness
There is a legal duty for hospitals to plan and prepare for major incidents laid out by the Civil Contingencies Act 2004, which provides a framework for civil protection in the UK. The Act divides local responders into two categories, imposing a different set of duties on each.
Those in Category 1 are organisations at the core of the response to most emergencies (the emergency services, local authorities, NHS bodies). Category 1 responders are subject to the full set of civil protection duties. They will be required to:
- Assess the risk of emergencies occurring and use this to inform contingency planning
- Put in place emergency plans
- Put in place business continuity management arrangements
- Put in place arrangements to make information available to the public about civil protection matters and maintain arrangements to warn, inform and advise the public in the event of an emergency
- Share information with other local responders to enhance co-ordination
- Co-operate with other local responders to enhance co-ordination and efficiency
- Provide advice and assistance to businesses and voluntary organisations about business continuity management (local authorities only)
Category 2 organisations (the Health and Safety Executive, transport and utility companies) are ‘co-operating bodies’. They are less likely to be involved in the heart of planning work but will be heavily involved in incidents that affect their own sector. Category 2 responders have a lesser set of duties – co-operating and sharing relevant information with other Category 1 and 2 responders.
Frontline response at a disaster scene
The scene commanders are known as ‘incident officers’; each service present at the incident will have its own incident officer:
- Police Incident Officer (PIO)
- Ambulance Incident Officer (AIO)
- Fire Incident Officer (FIO)
- Medical Incident Officer (MIO)
The Police have overall responsibility for the scene, and the PIO is, therefore ‘in overall control’.
The Ambulance Service are often the earliest responders present at the scene of the incident. A senior crew member will be designated as the AIO. The AIO will usually be in charge until a more senior officer arrives, and will be responsible for:
- Assessing the situation at the scene
- Declaring a major incident and giving a situation report (SITREP)
- Deciding where to establish the Control Point, the Casualty Clearing Station (CCS), and the Ambulance Parking Point
- Planning entry and exit routes for ambulances
- Communication with all health service personnel at the scene
- Holding discussions with the chain of command about the need for additional support and equipment.
There will usually be many ambulances at the scene, but the control vehicle can be recognised as the one that still displays its flashing blue lights. Following a handover from the AIO, the MIO will take over managerial responsibility for the deployment of health service personnel at the scene and will liaise closely with the AIO to ensure that there is effective management of resources.
Reporting a major incident
The METHANE mnemonic is now the recognised standard model for passing incident information between services and their control rooms when reporting a major incident:
- Major incident declared
- Exact location
- Type of incident
- Hazards present and suspected
- Access – routes that are safe to use
- Number, type, and severity of casualties
- Emergency services now present and those required.
The Medical Emergency Response Incident Team (MERIT)
The Medical Emergency Response Incident Team (MERIT), formerly known as the Mobile Medical Team, forms an integral part of the NHS response to major, mass casualty and significant incidents, providing advanced medical advice at a range of emergency incidents. The team usually consists of a doctor and a nurse, or two of each. Ideally, they should not come from the hospital that will be receiving casualties, as they need all their staff but, in a remote area, this may not be practical.
When the MERIT arrives at the scene, they should report to the MIO. They are usually sent to the CCS but may be required to assist with the triage and treatment of entrapped casualties.
Command structure
The gold-silver-bronze hierarchy is used for the command structure at the scene of a major incident in the UK.
Gold (Strategic):
The Gold Commander is in overall control of their organisation’s resources at the incident. They are located at a distant location, called the Gold Command. The Gold Commanders for each organisation are usually co-located, but if this is not possible, they should be in constant communication with each other.
Silver (Tactical):
The Silver Commander for each organisation is the senior member of each service present at the scene of the major incident. They are responsible for managing the resources available at the scene so that the strategic aims of the Gold Commander can be achieved. They work closely with the Silver Commanders of other organisations and are not directly involved in dealing with the incident itself.
Bronze (Operational):
The Bronze Commander directly controls their organisation’s resources at the incident. They work with their staff on the scene of the incident. If an incident is widespread geographically, a number of Bronze commanders may assume responsibility for different areas. In complex incidents, Bronze commanders may share tasks or responsibilities.
Organisation at the scene
The Police and Fire Service will cordon off the scene, and no one can enter without permission from the appropriate officer. Silver and Bronze areas are set up at the scene of the major incident.
The Silver area is located within an outer cordon that surrounds the inner cordon. The CCS, Ambulance Parking Point and each organisation’s service incident commanders are located here. Medical personnel will only enter the Silver area if instructed to do so by the MIO and if permitted to do so by the service responsible for safety at the scene. This is usually the Fire Service. Primary triage, the evacuation of casualties and the treatment of trapped casualties occurs here.
The Bronze area is located within an inner cordon that surrounds the scene of the incident. All medical activity within the Bronze area is directed by the MIO and AIO, working together. Doctors are under the command of the MIO, and ambulance personnel are under the command of the AIO.
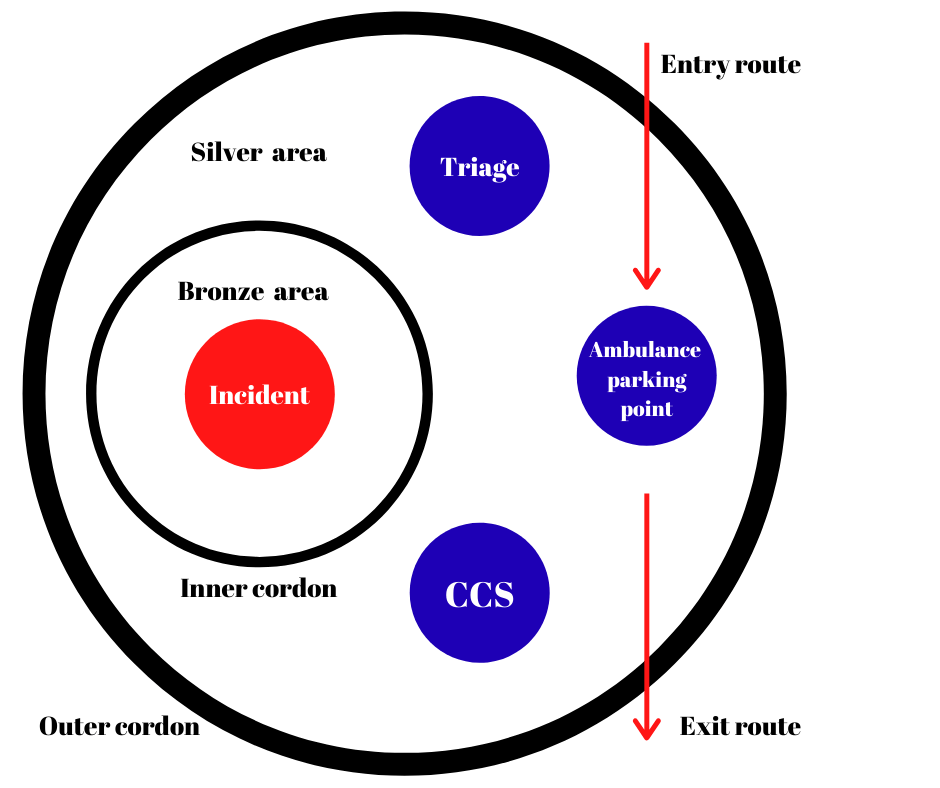
Image © Medical Exam Prep
Triage
Triage is the process of determining the priority of patients’ treatment based upon the severity of their condition and their likelihood of recovery. It enables limited resources to be deployed efficiently, allowing as many lives as possible to be saved.
In the setting of a major incident, priorities are numbered 1 to 3 in descending order of need, and are colour-coded as follows:
- P1: Immediate priority. This applies to those who will die without immediate life-saving intervention. Colour code red.
- P2: Intermediate priority. This group will also need significant interventions but can wait a few hours. Colour code yellow.
- P3: Delayed priority. They will need medical treatment, but this can safely be delayed. Walking wounded are automatically classified as P3. This is related to the motor score on the Glasgow Coma Scale and predicts a favourable outcome. Colour code green.
- Dead is the fourth classification and is important to prevent the expenditure of limited resources on those who are beyond help. Dead bodies should be left where they are, partly to avoid unproductive use of resources and partly because this may be a crime scene. Colour code black.
Next: Major Incident Management Part 2 – At the Hospital
Header image used on licence from Shutterstock
Thank you to the joint editorial team of www.mrcemexamprep.net for this ‘Exam Tips’ blog post.